The air inside a negative pressure hospital room does not move like normal air. It pulls. It whispers against the seals of heavy double doors, a constant, mechanical inhalation designed to keep the microscopic world of the inside from escaping to the outside. For those standing on the sterile side of the glass, that soft, persistent hum is the sound of a barrier holding.
On a rainy Tuesday evening in England, that hum became the loudest noise in the building.
A patient had arrived. They possessed a history of recent travel to a region in Africa currently battling an uptick in cases of Ebola viral hemorrhagic fever, and more importantly, they possessed a temperature that was climbing. In the cold language of public health briefings, this is known as a suspected case under investigation. In the warm, fragile reality of a hospital ward, it is a human being shivering under a crisp white sheet, watching a doctor pull on layers of synthetic defense, wondering if their own blood has turned against them.
Fear travels faster than any pathogen. It crosses oceans in the span of a single headline. When news broke that a British hospital was testing an individual for Ebola, the collective memory of the 2014 West African epidemic flared instantly. We remember the images of hazmat suits, the stark burial teams, and the terrifying speed of transmission. But panic obscures the actual architecture of modern medicine. It hides the quiet, disciplined choreography that takes place when the system is forced to look an ancient threat in the eye.
The Sound of Two Negative Pressure Doors Closing
To understand what happens in these moments, you have to look past the sensationalism. Consider the routine. A traveler returns to the United Kingdom, perhaps landing at Heathrow or Gatwick, carrying nothing more unusual than jet lag and a few souvenirs. Then, twenty-four hours later, the muscle aches begin.
Fatigue. A dry throat. A headache that feels like a spike driven behind the eyes.
In ninety-nine cases out of a hundred, this is malaria, or dengue, or a severe strain of influenza picked up in transit. The human body is an exquisite machine, but it is easily disrupted by travel. Yet, because of where this traveler has been, a silent tripwire is tripped the moment they call emergency services or walk into an emergency department.
The protocol is immediate. It is unyielding.
The patient is isolated not because there is certainty, but because there is no room for error. The medical staff who step into that room do not do so lightly. They dress in pairs, checking each other’s suits for the tiniest gap, the smallest sliver of exposed skin. Every seam is taped. Every breath is filtered through a respirator. Inside the suit, it is hot, humid, and remarkably lonely. Your own breath echoes in your ears. You look at your colleague through a plastic visor, communicating with nods and deliberate, slowed-down hand gestures.
Then you walk through the first door. It closes behind you with a heavy, pneumatic thud. You wait in the anteroom, letting the pressure stabilize, before opening the second door to face the patient.
This is where the abstract reality of global health statistics becomes deeply personal. The person in the bed is not a statistic. They are terrified. They see figures approaching them that look less like healers and more like astronauts exploring a hostile planet. The first duty of the physician in that moment is not biological; it is psychological. You have to speak through a thick filter, raising your voice just enough to sound human, reassuring someone whose mind is likely racing toward the worst possible conclusion.
The Math of an Invisible Border
We like to think of borders as solid lines on a map, guarded by passport control and customs agents. The truth is much more fluid. In an era of commercial aviation, every city on Earth is less than thirty-six hours away from any other city. A virus does not recognize a passport. It does not wait for permission to board.
When health officials note that Ebola cases are rising in specific provinces of Africa, the response in London or Manchester cannot be indifferent. The network is too tight.
Consider the mechanics of the virus itself. Ebola is not influenza; it does not drift through the air on a casual cough across a crowded subway car. It requires direct contact with bodily fluids. This biological fact is both a relief and a challenge. It means that casual transmission in a supermarket or a terminal is highly unlikely. But it also means that those who care for the sick—family members and healthcare workers—are the ones who stand directly in the line of fire.
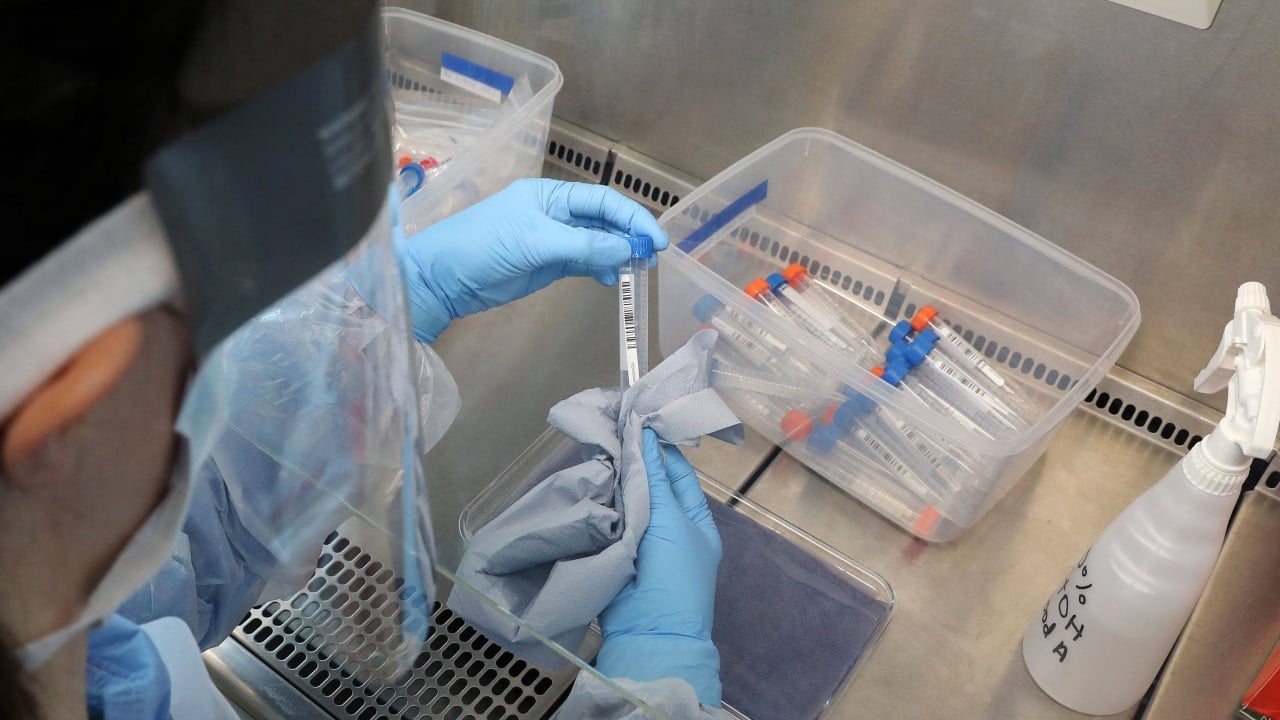
The testing process itself is a masterclass in controlled tension. A blood sample is drawn with extreme care, the needle disposed of in a specialized container that will later be incinerated at temperatures high enough to melt steel. The vial is wrapped in multiple layers of protective packaging, placed inside a crush-proof transport container, and sent via a dedicated courier to a high-containment laboratory.
Then, the waiting begins.
PCR testing can detect the genetic material of the virus within hours, but those hours feel like days for everyone involved. For the patient, it is a period of profound isolation. For the public, it is an uncomfortable reminder of our shared vulnerability. We realize, with a sudden jolt, that our safety is entirely dependent on the integrity of a few individuals following a checklist in a sealed room.
Inside the Isolation Chamber
What does it feel like to wait for a result that could change the trajectory of your life?
Imagine looking at your hands, wondering if the cells inside them are replicating a pathogen that has a historic mortality rate of up to ninety percent in some outbreaks, though modern therapeutics have significantly lowered that figure when administered early. You cannot touch anyone. Your food is brought in on disposable trays that are destroyed immediately after use. Your only window to the world is a pane of reinforced glass or the screen of a smartphone that you must constantly wipe down with disinfectant.
The skepticism of the modern observer often leads to a desire for absolute certainty. We want the test to be instant. We want the danger to be zero.
But medicine is an art of managing probabilities, not absolute guarantees. While the public waits for a press release, epidemiologists are already backward-mapping the patient’s movements. Who sat next to them on the flight? Which taxis did they take? Did they visit a local clinic before being transferred to the specialist unit? This is the invisible labor of public health—contact tracing that begins long before a positive result is confirmed, just in case the worst-case scenario becomes reality.
It is a grueling process of phone calls, flight manifests, and quiet conversations. It is done without fanfare, usually without the public ever realizing it happened. If the test comes back negative, the machinery slows down, the suits are discarded, and the world moves on to the next news cycle. The patient is treated for whatever standard infection actually caused their fever, and the system resets.
But the exercise is never a waste of time. It is a live-fire drill for a war that never truly ends.
The Anatomy of Panic vs. The Reality of Protocol
Every time a suspected case arises in a Western nation, a predictable rhythm of anxiety ripples through social media and tabloid journalism. Headlines lean heavily on words that evoke dread. There is a temptation to view the situation as a failure of containment, a breach of the fortress.
This perspective gets the story completely backward.
The fact that a suspected case is identified, isolated, and tested within hours of presentation is not evidence of a failing system; it is evidence of a system that is working exactly as designed. The trigger points are calibrated to be incredibly sensitive. It is far better for a hospital to isolate fifty patients with standard tropical illnesses than to miss a single case of a high-consequence infectious disease.
The true danger lies not in the occasional imported case that enters a highly prepared clinical environment. The real problem lies elsewhere, thousands of miles away, where the health systems are underfunded, where clinics lack basic personal protective equipment, and where communities are distrustful of external medical intervention because of historical trauma or misinformation.
When we look at the rising numbers in Africa, the correct response is not to pull up the drawbridge and hope the moat is wide enough. The moat does not exist. The only effective defense against a global health threat is the strengthening of the front lines where the virus originates. This means supporting local doctors, funding rapid diagnostic tools in rural clinics, and ensuring that when a outbreak begins, it can be smothered at the source rather than chased around the globe.
An Unbroken Thread
Late in the night, the laboratory results finally arrive. The paperwork is cleared. The digital signature of the consultant virologist appears on the hospital network.
Negative.
A collective breath is released across the department. The tension that had held the ward in a vice grip for twelve hours dissipates like morning mist. The negative pressure doors still hum, but the urgency is gone. The suits are taken off according to a strict, multi-step decontamination sequence, each piece of plastic peeled away with careful movements to ensure no surface touches the skin.
The patient will recover. They will go home to their family, their fever managed, their name remaining anonymous, a brief footnote in a weekly epidemiological report.
But as the hospital returns to its normal nightly rhythm—the soft squeak of nurses’ shoes on linoleum, the distant beep of heart monitors, the low murmur of the emergency department down the hall—the lesson remains. We are bound to each other by an unbroken thread of biology. The health of a village in a remote province is intimately connected to the safety of a suburb in an English city.
We cannot afford to look away when a crisis happens elsewhere, assuming it will stay confined to the map. The hum of the isolation room is a reminder that the world is small, the stakes are infinite, and our survival depends entirely on our willingness to care for the stranger at the gate, long before they ever reach the door.


